Digital technology has changed the way we practice dentistry. It has raised our clinical skills and standards, made work more fun, and raised the value of dentistry in our patients' eyes. Digital scanning, design, and chair side milling and 3D printing provides tremendous improvements in speed, accuracy, efficiency, and quality. It has also created possibilities for increased revenue and decreased costs. However, digital dentistry also comes with new challenges, unique learning curves, and varying opinions regarding design and final outcome of restorations and appliances. In this series of blogs, I will focus on different types of appliances and their indications and design to help the clinician develop a simple step-by-step approach to diagnosis, treatment planning, and appliance design for various types of para-functional conditions utilizing the 3Shape Trios intra-oral scanner, 3Shape Splint Studio, and the Formlabs 3D printer.
Anytime one is treating and designing appliances for patients in order to manage or treat a para-functional habit, it is important to understand which type of appliance to fabricate. Before using the 3Shape intraoral scanner, it’s critical to determine whether the patient has a muscle problem or a joint problem. Appliance choice is determined by joint and muscle condition and establishing which one is the problem in each particular case will impact the way we design the appliance.
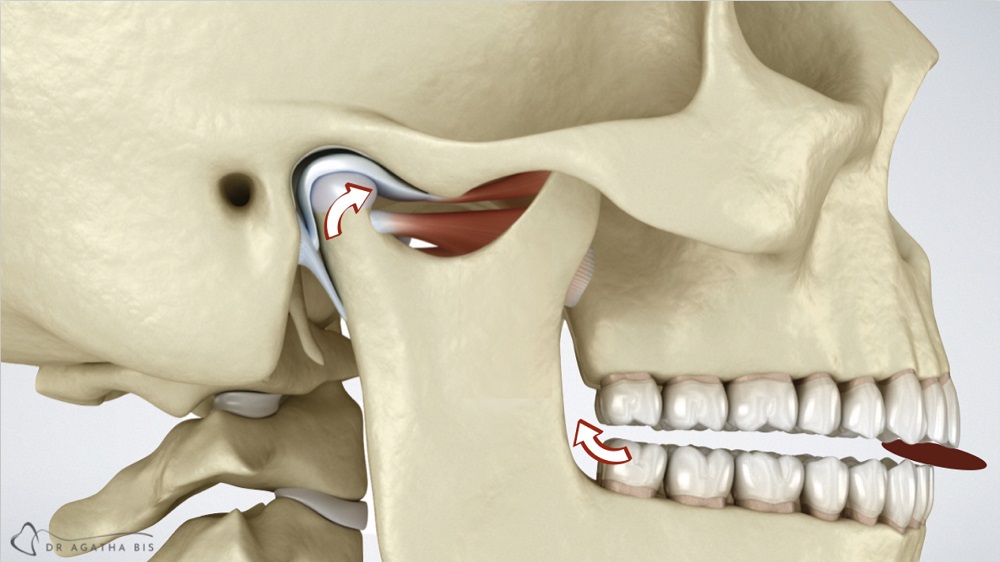
A simple way to determine whether it’s a muscle issue or a joint issue it through the use of a leaf gauge. Loading the joint by having the patient bite down on a leaf gauge is effective because anterior contact (only) loads the joint at 60% of the bite force. That means that when front teeth contact, they apply all the bite force and seat the joint up into the socket. If a joint is not healthy, it won’t like it. In contrast, the second molar contact creates only 5% of the joint load because it’s so close to the middle. That’s essentially what anterior-only appliances do: they increase joint loading if muscle activity doesn’t decrease. And this type of appliance can be effective for a clencher… but not every clencher is purely a clencher so we need to be really careful with these types of appliances.
If a patient has a displaced disc, we want to avoid joint loading and an anterior load appliance would be contra-indicated.
How do we establish what’s happening and which appliance is best?
Check out the next blog in this series.
– Written by Dr. Agatha Bis
 Book your cosmetic consultation in Oakville
Book your cosmetic consultation in Oakville
 Visit us at smilesbybis.com
Visit us at smilesbybis.com
 Call us at (905) 338-6684
Call us at (905) 338-6684